Adult Day Care Activity Ideas to Keep Clients Engaged
Adult day care centers provide a vital service, offering a ...
 Last year, a home care agency owner named Linda got an unexpected call from the state Medicaid office. Her agency had just expanded into a new state, and she was informed that unless she started sending Electronic Visit Verification (EVV) data through the state’s approved aggregator, she’d be out of compliance and could risk losing Medicaid reimbursement.
Last year, a home care agency owner named Linda got an unexpected call from the state Medicaid office. Her agency had just expanded into a new state, and she was informed that unless she started sending Electronic Visit Verification (EVV) data through the state’s approved aggregator, she’d be out of compliance and could risk losing Medicaid reimbursement.
Like many agency owners, Linda was already using an EVV-compliant software for scheduling and visit tracking. But what she didn’t realize was that each state has different rules and in this new state, all EVV data had to be funneled through a third party: the EVV aggregator.
This blog is written for home care providers like Linda. Whether you’re expanding across state lines or just trying to understand what an EVV aggregator does, this guide is here to simplify it.
At its core, an EVV aggregator is a data clearinghouse. It’s a state-approved system that collects EVV data from different software vendors and ensures that this data complies with state and federal guidelines. Once the data is validated, it is passed along to Medicaid or used to support audits and compliance checks.
Think of the aggregator like a toll booth on a highway. Every vehicle (EVV data) must pass through it before continuing. If the vehicle doesn’t have the right credentials or information, it gets turned away—or flagged for follow-up.
EVV became mandatory under the 21st Century Cures Act, which required states to electronically verify:
While this act applied to personal care services (PCS) and home health services (HHCS), the implementation details were left to each state. Some states chose an open model—allowing agencies to use their own EVV vendors, while others imposed a closed or hybrid model.
States using the open model needed a way to standardize incoming data from dozens of different systems. Enter the EVV aggregator.
Not all EVV setups are created equal; discover why many agencies prefer the flexibility and power of a 3rd-party software solution.
While Electronic Visit Verification (EVV) is federally mandated under the 21st Century Cures Act, each state has adopted its own approach to implementation. This includes selecting an EVV aggregator—a system that collects, validates, and forwards visit data to the state Medicaid program.
Most states fall into one of the following EVV models:
Each aggregator—such as Sandata, HHAeXchange, Tellus, or CareBridge—has its own data formats, validation rules, and submission protocols. For example, Sandata often requires JSON-formatted data, while HHAeXchange prefers flat file uploads.
Selecting the right EVV vendor is crucial, especially if your agency operates across multiple states. Some vendors (like Ankota) offer multi-state integration capabilities, which can help ensure compliance no matter where your services are delivered.
Below is a detailed table showing each state's EVV aggregator, the model they use, and Ankota's integration status for that environment:
| State | EVV Aggregator | EVV Model | Ankota Integration |
|---|---|---|---|
| Alabama | Sandata | Closed | Supported |
| Alaska | TBD | TBD | Pending |
| Arizona | Sandata | Open | Supported |
| Arkansas | Tellus | Closed | Supported |
| California | Sandata | Open | Supported |
| Colorado | Sandata | Open | Supported |
| Connecticut | Sandata | Open | Supported |
| Delaware | Sandata | Open | Supported |
| Florida | HHAeXchange | Closed | Supported |
| Georgia | Tellus | Closed | Supported |
| Hawaii | TBD | TBD | Pending |
| Idaho | TBD | TBD | Pending |
| Illinois | Sandata | Open | Supported |
| Indiana | Sandata | Open | Supported |
| Iowa | Sandata | Open | Supported |
| Kansas | Sandata | Open | Supported |
| Kentucky | Sandata | Open | Supported |
| Louisiana | Sandata | Open | Supported |
| Maine | Sandata | Open | Supported |
| Maryland | Sandata | Open | Supported |
| Massachusetts | Sandata | Open | Supported |
| Michigan | Sandata | Open | Supported |
| Minnesota | Sandata | Open | Supported |
| Mississippi | Sandata | Closed | Supported |
| Missouri | Sandata | Open | Supported |
| Montana | TBD | TBD | Pending |
| Nebraska | Sandata | Open | Supported |
| Nevada | Sandata | Open | Supported |
| New Hampshire | TBD | TBD | Pending |
| New Jersey | HHAeXchange | Closed | Supported |
| New Mexico | Sandata | Hybrid | Supported |
| New York | Sandata | Closed | Supported |
| North Carolina | HHAeXchange | Closed | Supported |
| North Dakota | TBD | TBD | Pending |
| Ohio | Sandata | Open | Supported |
| Oklahoma | Sandata | Open | Supported |
| Oregon | Sandata | Open | Supported |
| Pennsylvania | HHAeXchange | Open | Supported |
| Rhode Island | Sandata | Open | Supported |
| South Carolina | Tellus | Closed | Supported |
| South Dakota | Sandata | Open | Supported |
| Tennessee | CareBridge | Closed | Supported |
| Texas | TMHP | Open | |
| Utah | Sandata | Open | Supported |
| Vermont | TBD | TBD | Pending |
| Virginia | Sandata | Open | Supported |
| Washington | Sandata | Open | Supported |
| West Virginia | Sandata | Open | Supported |
| Wisconsin | Sandata | Open | Supported |
| Wyoming | TBD | TBD | Pending |
Let’s go back to Linda’s story.
When she entered a new state, she was still using her existing EVV software. But because that state required data to flow through Sandata, she had to find a way to integrate. Her vendor didn’t yet support that state’s Sandata feed. So, Linda had to either switch vendors, manually upload visit files, or work with a third-party integration specialist.
This led to delays, billing issues, and extra administrative overhead. And this isn’t unique to Linda. Many providers run into similar issues when they expand into new markets or when states update their aggregator requirements.
Ready to find a vendor that integrates seamlessly with state aggregators? Here are the top 10 solutions currently leading the industry.
Here’s the good news: you don’t have to do all this alone.
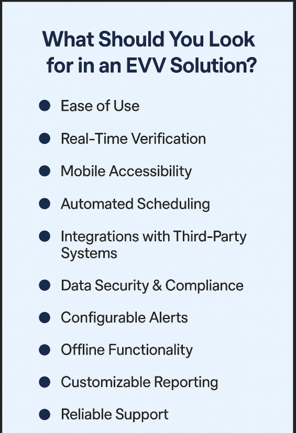
If you’re evaluating EVV software or considering expanding your service area, make sure to ask your vendor:
Ideally, your software should integrate directly with all relevant state aggregators and alert you immediately if anything fails.
Understand your state’s model: Open, closed, or hybrid? Know what kind of aggregator (if any) your state uses.
Use a vendor that supports multi-state compliance, especially if you plan to expand.
Set up automated reports: Make sure your system tracks successful and failed submissions.
Train your team: Everyone, from schedulers to billing, should understand how EVV data flows.
Don’t ignore rejections: A rejected visit isn’t just a delay—it could mean lost revenue or compliance risks.
If you're working within the HHA Exchange ecosystem, make sure you choose a partner that is fully compatible and compliant.
EVV compliance may seem like just another checkbox, but it’s become a critical part of getting paid and staying in good standing with Medicaid. EVV aggregators are a necessary part of that process, especially for providers in open states.
At Ankota, we’ve helped providers just like Linda adapt to aggregator requirements across dozens of states. We handle the complex integrations so you can focus on care, not file formats.
If you’re struggling to understand how your EVV data connects to the state, you’re not alone, and we’re here to help.
Want to learn more about how Ankota integrates with EVV aggregators across the U.S.? Let’s talk.
Ankota's mission is to enable the Heroes who keep older and disabled people living at home to focus on care because we take care of the tech. If you need software for home care, EVV, I/DD Services, Self-Direction FMS, Adult Day Care centers, or Caregiver Recruiting, please Contact Ankota.

Vijay is an expert on all-things Home Care and Electronic Visit Verification (EVV). He serves as the VP of Sales for Ankota
.png)
.png)
.png)


Trusted by home care agencies nationwide
