Adult Day Care Activity Ideas to Keep Clients Engaged
Adult day care centers provide a vital service, offering a ...
.png)
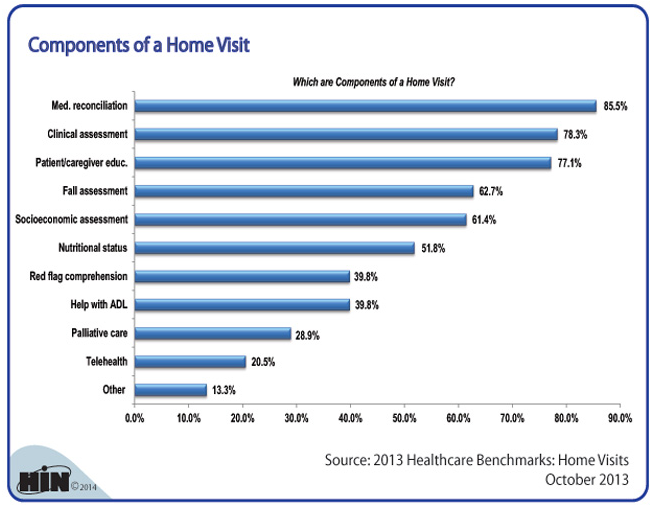
I found an interesting graphic on the website for the Healthcare Intelligence Network (www.hin.com) that itemizes the top components that occur in a home health visit.

The top 6 components, performed on more than half of the visits, in order, are as follows:
Here's a the full graphic:
What will this mix of Components Look like in 10 years?
Based on the change in health care to capitated payment structures, we believe that there will be new components on the list in the coming years. Some of the candidates are as follows:
At Ankota, we strongly believe that Home Health Agencies can be the critical factor that saves hundreds of billions of dollars per year in health care costs while providing better population health and higher patient satisfaction. To help with this, we've created software for HIPAA compliant care coordination, care transitions and ongoing care. Click on one of the images below to learns more.


Ankota provides software to improve the delivery of care outside the hospital, focusing on efficiency and care coordination. Ankota's primary focus is on Care Transitions for Reeadmisison avoidance and on management of Private Duty non-medical home care. To learn more, please visit www.ankota.com or contact Ankota.

Ken is the founder and CEO of Ankota, a company that helps any organization that helps older or disabled people live independently in their home of choice. Having grown up with a disability and a passion for healthcare, this is Ken's mission
.png)
.png)



Trusted by home care agencies nationwide
