Adult Day Care Activity Ideas to Keep Clients Engaged
Adult day care centers provide a vital service, offering a ...


We recently created a series of tutorials intended for folks in Virginia but that also serve as a useful tutorial for folks outside of Virginia as well. With that in mind, I'm sharing it here for our Ankota blog readers.
Though the information below does reference specific forms, it provides helpful information about creating an electronic care plan in general. Because of that, it is applicable to a broader audience.
Take a look below and let us know what you think:
In some states, like Missouri, your authorizations come with a specific set of care plan tasks that are created by an independent assessor. The assessor determines that tasks that the client needs and they use that to determine how many units of care to authorize.
In other states, and in essentially all Private Duty Home Care organizations, there is an assessment process where a nurse, case manager, or supervisor visits the client and their family to evaluate their needs on a form (sadly it's usually on paper). These forms might be as simple as a list of the care plan items, but more often they're based on Activities of Daily Living (ADLs).
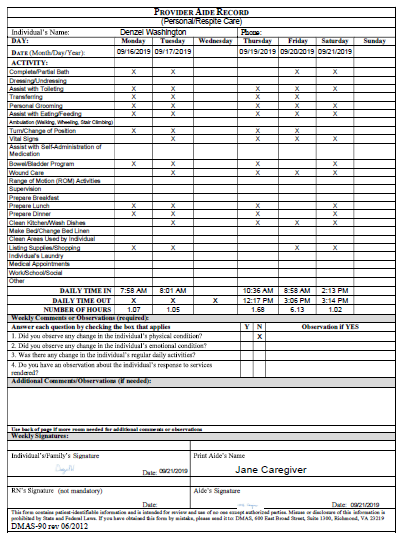
The best practice we're sharing today is to make the assessment into an electronic form, and have the form create the care plan. This is a best practice for the following reasons:If you're not in Virginia, you can just glance through this to get the gist, but to understand the concept, the form shown at the bottom (the DMAS-90) is the audit report showing what was done by the caregivers, but the care plan items relevant for this specific client are taken from the assessment form (the DMAS-97)
A lot of agencies have their nurse or supervisor fill out the DMAS-97 on paper and then someone in the office transcribes the information into the care plan items for the client. A best practice is instead to have an electronic version of the DMAS97AB filled out, and then once it's submitted, it creates the care plan automatically.
While this works well, there are a few specific recommendations we can offer, as follows:
The key takeaway for your agency is that regardless of your location, your home care software can be providing a paperless solution that ties your forms to your clients. At Ankota, we've even developed a mobile app so that the forms can be filled in off line.
For help with your EVV implementation, please feel free to click here!
\Ankota provides software to improve the delivery of care outside the hospital, focusing on efficiency and care coordination. Ankota's primary focus is on Care Transitions for Readmission avoidance and on management of Private Duty non-medical home care. To learn more, please visit www.ankota.com or contact us

Ken is the founder and CEO of Ankota, a company that helps any organization that helps older or disabled people live independently in their home of choice. Having grown up with a disability and a passion for healthcare, this is Ken's mission
.png)
.png)
.png)


Trusted by home care agencies nationwide
